Ebola vaccine development has made remarkable progress over the past decade. With the rise of licensed vaccines and real-world protection data, it has now become one of the major success stories in outbreak medicine. Vaccines against one of the deadliest epidemics in Zaire, Zaire ebolavirus, are now available. At the same time, scientists still face important challenges, including limited protection against all Ebola species, concerns about long-term protection, and the difficulty of testing vaccines due to unpredictable nature of outbreaks (Henao-Restrepo et al., 2016).

The progress of Ebola vaccine development
The biggest breakthrough in Ebola vaccine development came with rVSV-ZEBOV vaccine, commercially known as Ervebo, which showed strong efficacy, an estimated 100% efficacy, in the Guinea ring-vaccination trial in 2015-16 and later demonstrated real-world value during outbreaks. The strategy was based on vaccinating contacts of confirmed Ebola patients, and contacts of those contacts, creating a protective “ring” to help stop transmission in outbreak settings. Later, in 2018-2020 Ebola outbreak in the Democratic Republic of Congo, the rVSV-ZEBOV vaccination gaiend its value and had approximately 98% effectiveness against Ebola virus disease in that outbreak setting, as the outbreak unfolded in conflict-affected areas where conventional public health measures were difficult to implement (Dean and Longini, 2022).
Another major step forward was the development of the two-dose heterologous Ad26.ZEBOV/MVA-BN-Filo regimen, also known as the Zabdeno-Mvabea platform. This approach broadened the vaccine landscape beyond a single platform and showed that prime-boost strategies can improve immune responses. The regimen is given in two doses 56 days apart, and designed more for preventive vaccination (CDC, 2024). As of the World Health Organization’s 2025 guidance, Ervebo remains the vaccine specifically recommended for outbreak response and is the only Ebola vaccine available through the global emergency stockpile (WHO, 2025).
Why Ebola Vaccines Work
Most Ebola vaccines target the virus’s surface glycoprotein, a key target for protective immune responses. By exposing the immune system to this glycoprotein in a controlled way, vaccines train the body to recognize the virus and respond more rapidly after exposure (Wolf et al., 2021). However, protection is not driven by antibodies alone. Research increasingly suggests that cellular immunity and other immune functions also matter. A 2024 study comparing several Ebola vaccine regimens found that vaccine-induced T-cell responses can persist for years, with memory responses detectable up to 60 months after vaccination in laboratory analyses. These findings are important because they help explain how vaccination may generate longer-term immune readiness beyond the immediate antibody response (Wiedemann et al., 2024).
Animal studies were also crucial in the development process. Before large human efficacy trials were possible, researchers used nonhuman primate models to test vaccine safety and protection. These studies gave the field confidence to move forward, especially under the constraints of the animal rule and outbreak-based trial designs (Malik et al., 2023).

The Challenges
Despite the progress, Ebola vaccine development still faces major difficulties.
1. Outbreaks are unpredictable
One of the biggest problems of Ebola virus disease is that outbreaks are unpredictable, which makes conventional large-scale vaccine trials hard to conduct. When cases are scattered or limited, it becomes difficult to measure vaccine efficacy using standard trial methods (Malik et al., 2023).
2. Current vaccines do not protect equally against all Ebola species
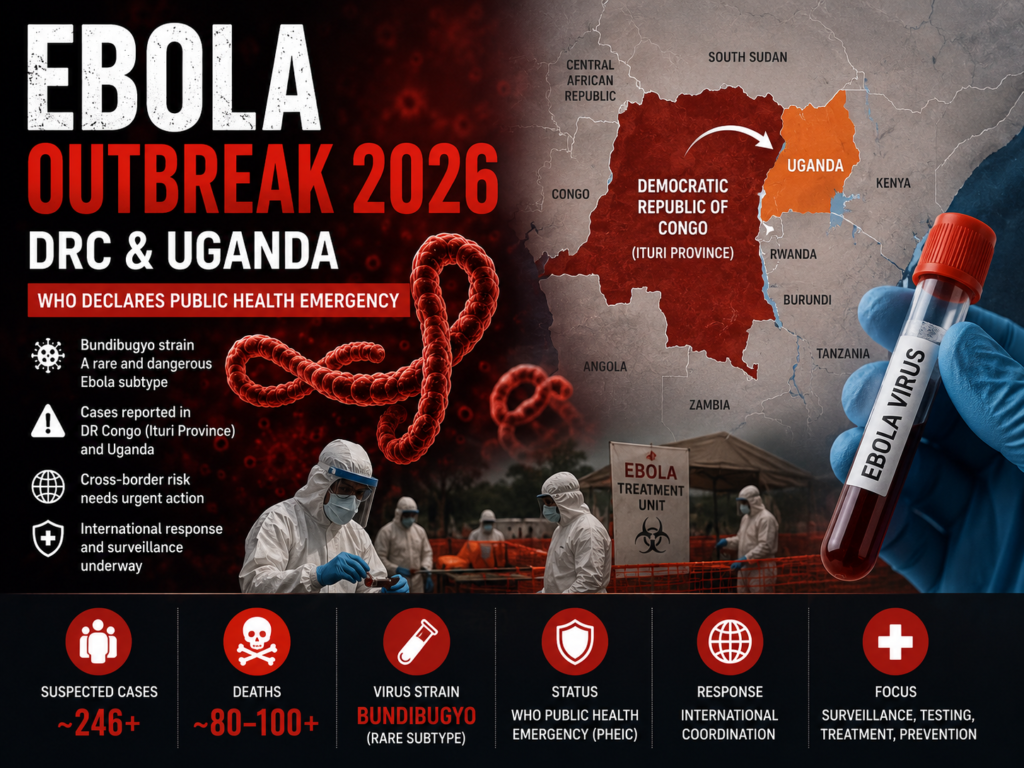
Viral diversity is another major challenge. Most successful vaccines target Zaire ebolavirus, but other species such as Sudan ebolavirus and Bundibugyo ebolavirus remain harder to protect against. As of 2026, there is no licensed vaccine specifically approved for Sudan virus or Bundibugyo virus outbreaks, although several candidates are in development and experimental options are being evaluated. This gap has become especially visible during recent outbreaks involving non-Zaire species (Jenkin et al., 2025).
3. Durability of protection remains a live research question
Another concern is durability. Some vaccines produce strong early immune responses, but protection may decline over time, making booster doses or prime-boost regimens important. A 2026 long-term follow-up study reported that the Ad26.ZEBOV/MVA-BN-Filo regimen induced immune responses lasting at least two years after the first dose, while other research has shown persistent cellular immune memory across multiple vaccine platforms (Manno et al., 2026).
4. Deployment is difficult in real outbreak settings
In addition, deployment in outbreak zones can be difficult. Ebola outbreaks often occur in areas affected by:
- conflict or insecurity
- weak transport systems
- shortage of trained health workers
- limited cold-chain infrastructure
- public mistrust or misinformation
These factors can slow contact tracing, delay vaccination, and reduce outbreak-control speed (Malik et al., 2023).
Safety and Real-World Use
Ebola vaccines have generally shown acceptable safety profiles in clinical studies and outbreak settings, but it remains an important part of vaccine evaluation. The rVSV-ZEBOV vaccine has been associated with short-term side effects such as fever, pain, and other reactogenic symptoms, which must be considered in mass vaccination programs. These events are usually temporary, but they matter for vaccine communication, especially during emergency campaigns.
Real-world studies have strengthened confidence in Ebola vaccination. Beyond reducing disease risk, one analysis of patients treated during the DRC outbreak suggested that prior rVSV-ZEBOV vaccination was associated with a substantially lower risk of death among those who later developed Ebola virus disease. This has made Ebola vaccination a key part of outbreak preparedness and response.
What comes next
The next phase of Ebola vaccine development is focused on making vaccines:
- better matched to immune correlates of protection, allowing researchers to predict performance more reliably
- broader, so they protect against multiple Ebola virus species
- longer-lasting, so protection does not depend on rapid outbreak-only deployment
- easier to distribute, especially in low-resource or conflict-affected areas (Flaxman et al., 2024)
In simple terms, the field has already achieved something extraordinary: Ebola vaccines now exist and can save lives. The next goal is to make them broader, stronger, and more practical for use in the toughest outbreak settings.
References
Henao-Restrepo, A. M., et al. (2017). Efficacy and effectiveness of an rVSV-vectored vaccine in preventing Ebola virus disease: Final results from the Guinea ring vaccination, open-label, cluster-randomised trial. The Lancet, 389(10068), 505–518.
World Health Organization. (2025). Ebola virus disease vaccines: Questions and answers.
Jenkin, D., et al. (2025). Safety and immunogenicity of a bivalent Ebola virus vaccine. The Lancet Microbe.
Dean, N. E., et al. (2022). The ring vaccination trial design for estimation of vaccine efficacy and effectiveness. Clinical Trials / PMC review.
CDC. (2024). Use of Ebola Vaccines — Worldwide, 2021–2023. MMWR, 73(16).
Wolf, J., et al. (2021). Development of Pandemic Vaccines: ERVEBO Case Study. Vaccines, 9(3).
Wiedemann, A., et al. (2024). Long-term cellular immunity of vaccines for Zaire Ebola virus disease. Nature Communications, 15.
Malik, S., et al. (2023). Ebola virus disease vaccines: Development, current status, and future challenges. Vaccines / PMC.
Manno, D., et al. (2026). Long-term safety and immunogenicity of the two-dose Ad26.ZEBOV/MVA-BN-Filo regimen. The Lancet Regional Health – Africa.
Flaxman, A., et al. (2024). Potent immunogenicity and protective efficacy of a multi-filovirus vaccine platform. PLOS Pathogens.
Pingback: History of Ebola: Discovery, Outbreaks and Timeline – Disease Buddy
Pingback: The Outbreak That Wouldn’t Die: Ebola – Disease Buddy
Pingback: Oxford Launches World’s First Human Trial of Bundibugyo Ebola Vaccine – Disease Buddy
Pingback: Ebola Outbreak Timeline: History, Major Epidemics and Global Impact (1976–2026) – Disease Buddy